Heat and Cold Therapy: Application of heat to relax muscles and improve blood flow, or cold to reduce inflammation and numb pain.
Electrical Stimulation:Techniques such as TENS (
Transcutaneous Electrical Nerve Stimulation) help to reduce pain by stimulating nerves.
Ultrasound Therapy:Ultrasound therapy uses sound waves to generate heat within tissues and promote healing.
Electrical Muscle Stimulation (EMS):EMS devices deliver electrical impulses to stimulate muscle contractions in specific muscle groups.
Interferential Current Therapy (IFT):Purpose: IFT involves using two high-frequency electrical currents that intersect and interfere with each other within the tissues.
Galvanic Stimulation (GS):Purpose: GS uses direct current (DC) to stimulate nerves and muscles.
Exercise Therapy:a) Strengthening Exercises: Focus on strengthening the core, lower back, and pelvic muscles to provide better support for the spine.
b) Stretching Exercises: Improve flexibility and reduce muscle tension in the lower back and
hamstrings.
c) Aerobic Exercises: Low-impact activities such as walking, swimming, or cycling to improve overall fitness without putting excessive strain on the back.
Manual Therapy:a) Spinal Manipulation: Gentle adjustments by the physiotherapist to improve spinal alignment and mobility.
b) Mobilization: Techniques to increase the range of motion in the affected joints.
c) Soft Tissue Massage: To reduce muscle tension and improve blood flow.
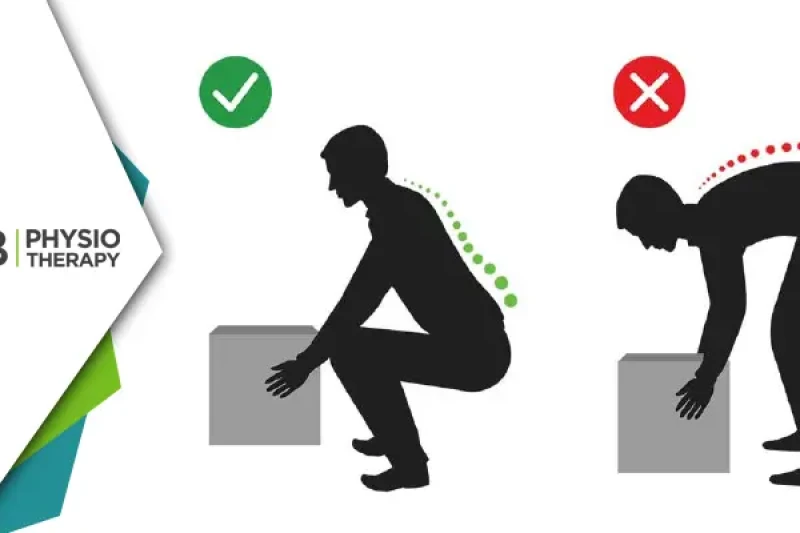
Postural Training:Ergonomic Advice: Guidance on maintaining proper posture during daily activities and using ergonomic furniture and devices.
Postural Exercises: Training to improve posture and reduce strain on the lower back.
Core Stabilization:Core Strengthening: Exercises to strengthen the muscles around the abdomen and lower back, which support the spine.
Functional Training:Functional Exercises: Activities designed to improve everyday movements and tasks, enhancing overall functionality and reducing pain during daily activities.
 Request a Callback
Request a Callback






 Request a Callback
Request a Callback