People often experience a dull ache, which changes to sharp or throbbing pain with activities such as getting up from a sitting position or prolonged sitting. While most people don’t know the actual cause of these symptoms, a condition called Coccydynia has often been linked to such chronic pains in the lower back. Identifying coccydynia and separating it from other types of lower back pain by Physiotherapists and Chiropractors is important for its pain management.
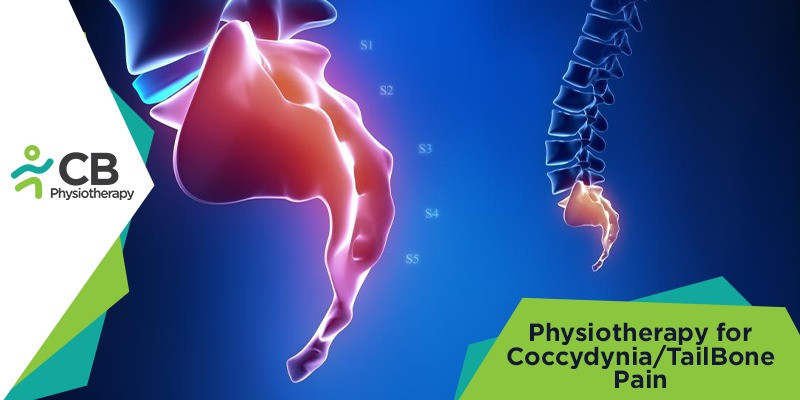
Coccydynia, or inflammation of the tailbone, is a unique type of lumbar pain that can cause patients a severe amount of discomfort and agony. Coccydynia/ Tailbone pain is a pain that occurs in or around the bony structure at the bottom of the spine (coccyx). The coccyx is much smaller than the sacrum, has an important weight-bearing role, and supports the body weight while sitting.
Physiotherapy has proven to be beneficial in teaching pelvic floor relaxation techniques (reverse Kegels) which help to get the coccyx into better alignment and can relieve the pain experienced when urinating or defecating. For women, tailbone pain can make menstruation uncomfortable as well. As women may suffer injury to the coccyx or direct trauma to the coccyx during childbirth, these conditions have been more commonly reported in females.
Common causes of Coccydynia:
Coccydynia/ Tailbone pain can be caused by trauma to the coccyx during a fall, prolonged sitting on a hard or narrow surface, degenerative joint changes, or vaginal childbirth. Tailbone pain ranges from a dull ache to a fierce stab. It can last for weeks, months, or sometimes longer. A diagnosis of coccydynia will usually identify one of the following underlying causes of pain:
Local trauma: direct injury to the coccyx is the most common cause of coccydynia. A fall on the tailbone can inflame the ligaments and injure the coccyx or the coccygeal attachment to the sacrum. Repetitive Strain Injury (RSI): Sports and activities that put prolonged pressure on the tailbone, such as horseback riding and sitting on hard surfaces for long periods of time or bicycling may cause the onset of coccyx pain.
Childbirth/ Pregnancy: During delivery, the pressure against the coccyx can sometimes result in injury to the coccygeal structures (the disc, ligaments, and bones. Some hormonal secretions during pregnancy may also soften the area between the sacrum and coccyx.
Referred to coccyx pain: In rare cases, the pain will be referred to the coccyx from elsewhere in the spine or pelvis, such as a lumbar herniated disc or degenerative lumbar disc
Physio-Therapeutic Approach
The initial goal of physiotherapy treatment is focused on providing postural education. A proper sitting posture ensures weight is taken off the coccyx and is instead loaded onto the ischial tuberosities and the thighs. Physiotherapists may also recommend the use of cushions. Modified wedge-shaped cushions (coccygeal cushions), help to relieve the pressure placed on the coccyx during sitting. Other treatment modalities include:Mobilizations: This can help realign the posture of the coccyx. Mobilization techniques may be the preferred technique when the goal of treatment is to increase coccygeal mobility.
Manipulation: Patients also find pain relief through manual manipulation of the coccyx. Through manual manipulation, the joint between the sacrum and the coccyx can be adjusted, potentially reducing pain caused by inadequate coccyx mobility.
Massage: Coccydynia may be reduced or alleviated by massaging tense pelvic floor muscles that attach to the coccyx. Tense muscles in this region can place added strain on the ligaments and sacrococcygeal joint, limiting its mobility or pulling on the coccyx.
TENS unit: Transcutaneous Electrical Nerve Stimulator (TENS) units apply electric stimulation that interferes with the transmission of pain signals from the coccyx to the brain. These devices can be a good option for patients who wish to keep their intake of medications to a minimum.
Dry needling: It is surprisingly comfortable and very effective for specific conditions such as pelvic pain, incontinence, coccyx pain (tailbone), and other diagnoses. It helps in reducing muscle spasms and assesses the mobility and position of the sacrococcygeal joint.
Although the vast majority of patients who seek medical attention respond to conservative treatments, some patients require more aggressive treatments. A multidisciplinary approach employing physical therapy, ergonomic adaptations, medications (NSAIDs), injections, and, possibly, psychotherapy leads to the greatest chance of success in the patients.
