
Chest physiotherapy is a process that includes clearance of secretions from large and small airways and re-expansion of the non-ventilated lung.
The objectives of chest physiotherapy are:
· To obtain outcomes equally and more effectively than bronchoscopy without the invasiveness, trauma, and risk of hypoxemia, complications physician involvement, and cost that bronchoscopy requires.
· To specifically, improve ventilation to areas of local lung obstruction.
· If the objectives of the chest physiotherapy are achieved, an increase in local lung expansion should occur and a parallel increase in perfusion to the affected area would result. If secretions are cleared from larger airways, airway resistance and now obstruction should decrease. Clearance of secretions and improve ventilation of small airways should increase lung compliance. If clearance of secretions from both large and small airways occurs, it is reasonable to assume that the work of breathing and oxygen consumption should decrease, and gas exchange improves.
Furthermore, if these objectives are achieved, the incidence of postoperative respiratory infection, morbidity, and hospital stay for those with acute and chronic lung diseases should be reduced.
Breathing exercises and ventilating techniques can take on many forms. Encompassed in the use of the term chest physiotherapy are the following maneuvers.
· Diaphragmatic breathing
· Incentive spirometry
· Segmental breathing: lateral costal expansion and posterior basal expansion
· Glossopharyngeal breathing
· Pursed lip breathing
· Postural drainage
· Percussion
· Vibration
· Coughing
· Suctioning
In addition, patient mobilization is used whenever possible.
· Diaphragmatic breathing: When the diaphragm is functioning effectively in its role as the primary muscle of inspiration, ventilation is efficient and the oxygen consumption of the muscles is very low during quiet relaxed breathing. When a patient relies on the accessory muscles of inspiration, the work of breathing increases. Although the diaphragm controls breathing at an involuntary level, a patient with a primary pulmonary disease such as chronic obstructive pulmonary disease
(COPD)can be taught breathing control by optimal use of the diaphragm and relaxation of accessory muscles. Controlled breathing techniques when emphasizing diaphragmatic breathing, are designed to improve the efficiency of ventilation decrease the work of breathing, increase the excursion of the diaphragm, and improve gas exchange and oxygenation. This technique is also used to mobilize lung secretions during postural drainage.
· Incentive Spirometry: Incentive spirometry involves an active maneuver toward maximal inspiration. It is a form of ventilation training that emphasizes sustained maximum inspiration. The patient inhales through a spirometer that provides visual or auditory feedback as the patient breathes in as deeply as possible.
· Lateral costal expansion: This type of breathing can be done unilaterally or bilaterally. Emphasizing deep breathing with a focus on the movement of this portion of the lower rib cage is thought to facilitate diaphragmatic excursion. It is a particularly useful technique for those patients with a stiff lower rib cage, as is often seen in the patient with chronic bronchitis, emphysema or asthma.
· Posterior nasal breathing: This form of segmental breathing is important for the postsurgical patient who is confined to bed in a semi-relining position for an extended period. Secretions often accumulate in the posterior segment of the lower lobes.
· Glossopharyngeal breathing: It is means of increasing a patient's inspiratory capacity when there is a severe weakness of the muscles of inspiration. It is taught to the patients who have difficulty taking in a deep breath for example in preparation for coughing. Most commonly taught to patients with high spinal cord injuries who can easily develop respiratory complications.
· Pursed lip breathing: Gentle pursed-lip breathing with controlled expiration is a useful procedure. It is thought to keep airways open by creating backpressure in the airways. It is taught to help a patient with chronic obstructive pulmonary disease (COPD) deal with episodes of dyspnea. Pursed lip breathing decreases the respiratory rate, increases the tidal volume, and improves exercises tolerance
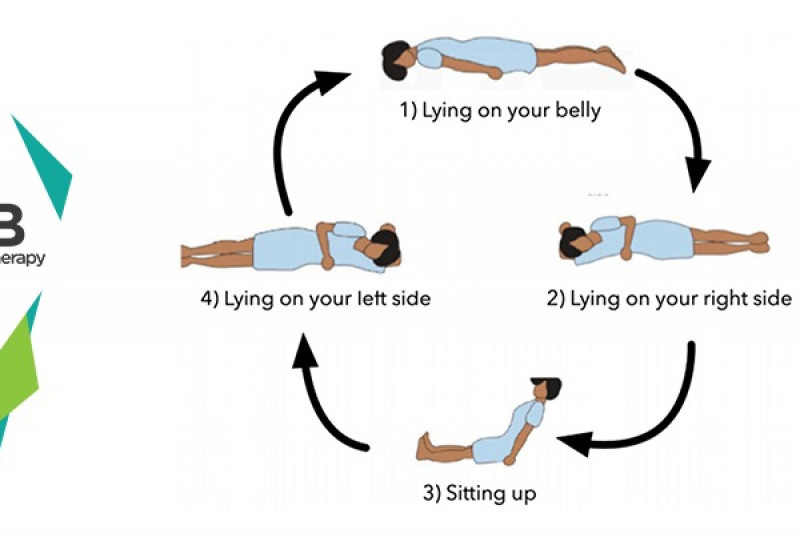
· Postural drainage: Postural drainage or bronchial drainage is a means of mobilizing secretions in one or more lung segments to the central airways by placing the patient in various positions so that gravity assists in the drainage process. When the secretions are moved to the large airways, they are then cleared by coughing or endotracheal suctioning. Postural drainage therapy also includes the use of manual techniques, such as percussion, and vibration as well as voluntary coughing. Modified positioning to avoid a head-down or fully horizontal position is necessary for most high-risk patients.
· Percussion: The percussion technique consists of rhythmic "clapping" with cupped hands over the involved lung segment. Percussion should produce a hollow sound, not a slapping sound. It should impart an energy wave transmitted through the chest wall to cause a loosening of bronchial wall secretions. The hand should create an "air cushion" on impact, which, it is proposed, aids in dislodging pulmonary secretions. Percussion is performed during both inspiration and expiration and should not result in undue pressure on the soft tissues of the chest. Manual percussion is normally performed at a rate of 100-480 times per minute and is reported to produce between 2 and 4 foot-pounds and 58 and 65 Newtons of force on the chest wall. Chest percussion should not cause undue pain to the patient and need not be forceful. If skin redness occurs with percussion, it is usually a result of improper technique, most commonly slapping or of not enough air being trapped between the hand and the chest wall. The trapped air creates the hollow cupping sound and is believed to be responsible for loosening the secretions.
· Vibration: Chest vibration, like percussion, is used in conjunction with postural drainage. Vibration is an intermittent chest wall compression performed primarily during expiration. It may be initiated just before the expiratory phase and extended to the beginning of the inspiratory phase. This technique can be used during voluntary or ventilator-controlled expiration and should be performed over the involved area of the lung. If vibration is performed on a spontaneously breathing patient encouragement toward a maximal inspiratory effort should precede chest wall vibration. Maximal inspiration is followed by shaking of the chest wall in the direction that the ribs and soft tissues of the chest normally move during expiration. Various sources describe different types of vibration as "rib springing" or "chest shaking." All are more or less vigorous forms of the same general technique, with "vibration" usually referring to a gentler, more oscillatory treatment than the other terms. Frequencies of 12- 20 Hz are reported for manual vibration.
· Mechanical vibrators and percussors: Mechanical percussors and vibrators were developed primarily to assist in the home care physiotherapy of patients with chronic pulmonary pathology. They are introduced into the intensive care unit, because these mechanical devices may produce vertical or rotary movements or a combination of both, some studies refer to them as vibrators and some as precussors.
· Coughing: Coughing is effective in the removal of foreign bodies or excessive quantities of sputum and when normal ciliary activity is absent. The cough mechanism provides the most rapid means of secretion clearance. Airway clearance is an important part of the management of patients with acute or chronic respiratory conditions. A normal cough consists of an inspiratory effort. Glottis closes. Abnormal muscles contract and the diaphragm elevates, causing an increase in intrathoracic and intra- abdominal pressures. Glottis opens and explosive expiration of air occurs.
· Suctioning: Endotracheal suctioning may be the only means of clearing the airways in patients who are unable to cough or huff voluntarily or after reflex stimulation of the cough mechanism. Suctioning is indicated in all patients with artificial airways. The suctioning procedure clears only the trachea and the mainstream bronchi.
· Positive expiratory pressure (PEP): PEP therapy is equivalent to standard chest physical therapy. It is an airway clearance method that is administered by applying a mechanical pressure device to the mouth. By breathing out with a moderate force through the resistance of the device, a positive pressure is created in the airways that help to keep them open. This positive pressure permits airflow to reach beneath the areas of mucus obstruction and to move the mucus toward the larger airways where it can be expectorated. This technique may be suitable for alert, cooperative children over the age of four.
It is indicated for the patients in who cough is insufficient to clear thick localized secretions.
· Asthma
· Chronic obstructive pulmonary disease
· Bronchitis
· Bronchiectasis
· Atelectasis
· Lung abscess
· Pneumonia
· Cystic fibrosis
· Emphysema
· Patients having difficulty in breathing
· Unstable vitals (blood pressure, pulse, SPO2, etc).
· Unstable angina, cardiac arrhythmias
· Recent myocardial infarction
· Lung tumor
· Suspected or known active pulmonary tuberculosis
· Bleeding
· Elevated intracranial pressure
· Head and neck injury
· Pulmonary embolism
· Rib fracture with or without flail chest
· Surgical wound
· Uncontrolled hypertension
· Subcutaneous emphysema
· Recent epidural anesthesia or recent epidural or intrathecal drug administration
· Recent skin grafts or flaps on the thorax
· Osteomyelitis of the thorax
· Osteoporosis of the thoracolumbar region
· Unconscious patient with an unprotected airway
· Acute abdomen (i.e., abdominal aortic aneurysm, hiatal hernia, or pregnancy)
· Recent spinal surgery (i.e., laminectomy)
· Bronchopleural fistula
Select your City to find & connect with our experts regarding Physiotherapy for Chest Physiotherapy
 Request a Callback
Request a Callback








 Request a Callback
Request a Callback