
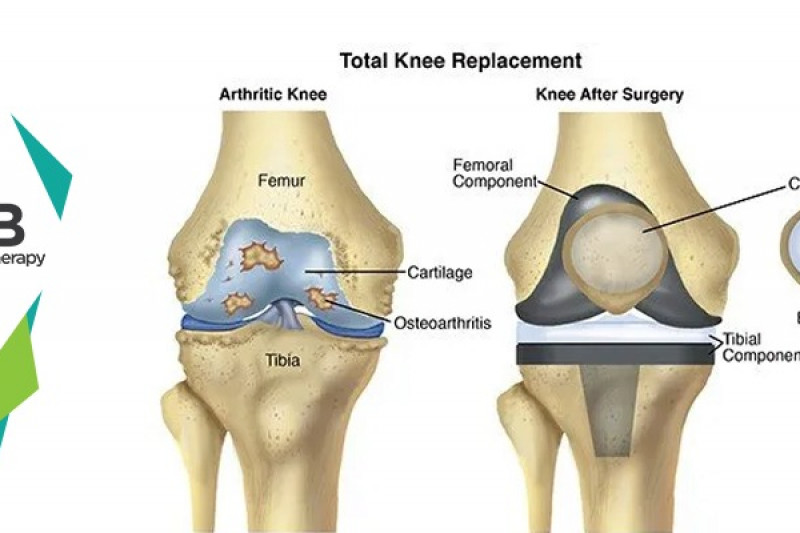
The semilunar cartilages are commonly called menisci and form an important shock-absorbing mechanism, which helps in the smooth functioning of the knee. They help in the gliding movement of the tibia on the femur.
The menisci are prone to injuries due to overload and overstretching. The other causes may be:
· Poor strength
· Poor flexibility
· Fatigue
· Imbalance
· Previous injury
· Overuse
These injuries are most commonly seen in:
· Athletes involved in soccer, football, kabaddi.
There are two menisci in a knee the medial menisci and the lateral menisci. The symptoms can be seen in anyone or both the menisci.
· Pain
· Tenderness
· Swelling
· Inflammation
· Locking of the knee
· Clicking sound
· Loss of knee movement
Pathology
There are three types of meniscal tears, longitudinal tear, horizontal tear, and oblique tear. Further longitudinal subtypes are bucket handle tear, posterior tear, and anterior tear.
Abduction external rotation violence, on the flexed weight-bearing knee, causes a tear in the medial meniscus. During football, it occurs when the player, standing on one leg which is slightly flexed at the knee, turns to tackle the ball with the other leg.
The lateral meniscus is damaged by the opposite violence i.e. internal rotation and abduction violence of the tibia on a semi-flexed weight-bearing knee.
Magnetic resonance imaging (MRI)
On Magnetic resonance imaging (MRI) acute injuries typically show up as the high signal intensity.
Plain radiographs
Plain radiographs should be obtained as the initial imaging modality to rule out a fracture, and evaluate any avulsion injuries.
Ultrasound
Ultrasound maybe used as a secondary tool to evaluate partial or complete tears
Special clinical tests
McMurray's test:
This test elicits a click of the cartilage if it is torn.
Apley's grinding test:
When the meniscus is torn, pain, and click localized to the joint line are elicited.
Bounce home test for bucket handle type tear:
If the extension is not complete or has a rubbery end-feel with elastic resistance to blocking full extension, it indicates bucket handle type of meniscal tear.
Oral non-steroidal anti-inflammatory drugs (NSAIDs) like naproxen, ibuprofen. Corticosteroid injection
(Medication not to be taken without doctor's prescription).
Techniques used by the physiotherapist:
· NMES:
Neuromuscular stimulations facilitate voluntary motor control and muscle strength.
Application of ultrasound decreases pain, increases range of motion, and decreases inflammation.
· Rest:
Short immobilization is advantageous in limiting the extent of damage at the site of the injury. Use of crutches and bed rest is important.
The physiological effects of ice are beneficial in the healing process should be applied in a plastic bag and wrapped directly over the affected area.
· Compression:
Gentle compression is used with a firm compressive bandage placed around the knee.
· Elevation:
Protection of the knee from the position of stress. It helps to reduce edema and allows the return of fluid to the heart, elevate the extremity above the heart level.
· Isometric exercises:
Isometric exercises for the quadriceps. These should be done at least for 5 minutes every hour. Prevention of quadriceps and reflex inhibition is important. The isometrics progressed slowly to the maximum and sustained for 10 -15 seconds, assist in strengthening the quadriceps, whereas speedy isometrics help in the resolution of edema and effusion.
· Ankle-toe movements:
When the leg is immobilized in a pop cast, vigorous movements to the ankle and toes are important to prevent venous thrombosis and to augment circulation.
· Heel slides:
Sit on a firm surface with a socks on the foot or a towel under the heel. Gently flex the knee with the foot approaching the buttocks, then return to the starting position.
· Wall slides:
Lie on a firm surface with the feet resting on the wall. Slowly begin to walk the feet down the wall.
· Straight leg raise (SLR):
SLR, straight leg raise should be initiated as an assisted movement. It can be made more effective by, slow repetitions with self-generated intramuscular tension without the heel making contact with the bed.
· Straight leg abduction (SLR modified to SLA):
SLA, straight leg abduction exercise has advantages of the two movements are that all-important muscle groups of the lower limb are exercised at the same time. Due to sustained contractions in all muscle groups, strength, as well as endurance, also improves to a great extent.
· Knee swinging:
Relaxed knee swinging should be made speedy with increased arc of movement to attain free mobility.
· Progressive resistive exercises(PRE):
Gradual self-resistive exercise with self-generated tension or graded resistance exercise with weight belts.
· Flexibility exercises:
Flexibility exercises of the static stretching using a 30-the second hold, relaxing, and performing 5 repetitions to hamstrings, iliotibial tract, and gastrocsoleus are important.
· Modified Straight leg raise (SLR):
By adding weight, the weight or resistance should be gradually progressive. The upper limit of resistance for the SLR should not be kept at 4.5 to 6.8kg. (as permitted by pain and achieved ROM, so as not to overstrain the knee.)
· Knee flexion:
Knee flexion exercises should be practiced in prone as well as on a static bicycle. Speed resistance and the seat height of the static bicycle should be properly adjusted so as not to overstrain the knee. Begin with a half-circle of the peddle. The session should be for 15 minutes initially, increasing gradually to an hour.
· Standing concentric isotonic exercises:
Stand near a table or wall for support. Place a cuff weight on the involved leg to bring the heel toward the buttocks in a slow controlled manner.
· Vigorous program:
When the pain is minimal, ROM and swelling are near normal. The endurance strengthening flexibility exercises are made progressive by suitable techniques. Progress to guided prone kneeling, assisted squatting, stair climbing and descending and cross leg sitting.
· Isokinetic exercises:
Isokinetic mode of exercise is effective in improving strength endurance and functional capacity of the quadriceps and hamstrings. It assists in improving ROM, due to the physiological overflow. As resistance is adjusted in relation to the muscle force through ROM, it prevents excessive compression of the joint. As the isokinetic provides fast contractile velocity, it improves control and coordination.
Aerobic exercises like running, jogging, and swimming can be initiated as the pain permits.
Select your City to find & connect with our experts regarding Physiotherapy for Meniscal Injury
 Request a Callback
Request a Callback





 Request a Callback
Request a Callback